
Page 52 - HPP ANTIMICROBIAL GUIDELINE 2018
P. 52
Suggested Treatment
Infection/Condition Comments
Preferred Alternative
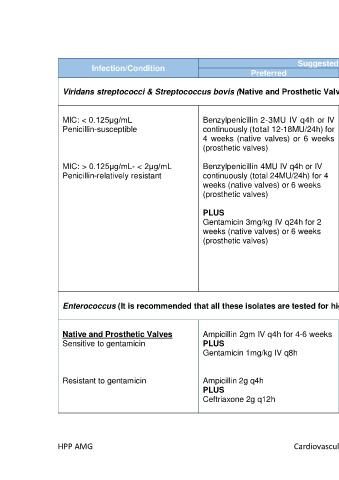
Viridans streptococci & Streptococcus bovis (Native and Prosthetic Valves)
MIC: < 0.125μg/mL Benzylpenicillin 2-3MU IV q4h or IV Ceftriaxone 2gm IV q24h for 4 weeks A 2-week treatment regimen that
Penicillin-susceptible continuously (total 12-18MU/24h) for (native valves) or 6 weeks (prosthetic includes gentamicin is reasonable in
4 weeks (native valves) or 6 weeks valves) patients with uncomplicated IE, rapid
(prosthetic valves) response to therapy, and no
underlying renal disease
MIC: > 0.125μg/mL- < 2μg/mL Benzylpenicillin 4MU IV q4h or IV Ceftriaxone 2gm IV q24h for 4 weeks
Penicillin-relatively resistant continuously (total 24MU/24h) for 4 (native valves) or 6 weeks (prosthetic For MIC >0.5 to <2ug/ml
weeks (native valves) or 6 weeks valves) Use gentamicin 1mg/kg IV q8h for 2
(prosthetic valves) weeks (native valves) or 6 weeks
PLUS (prosthetic valves)
PLUS Gentamicin 3mg/kg IV q24h for 2
Gentamicin 3mg/kg IV q24h for 2 weeks (native valves) or 6 weeks
weeks (native valves) or 6 weeks (prosthetic valves)
(prosthetic valves)
If unable to tolerate
penicillin/ceftriaxone:
Vancomycin 25-30mg/kg loading
dose then 15-20mg/kg IV q12h
Enterococcus (It is recommended that all these isolates are tested for high level resistance (HLR) to gentamicin)
Native and Prosthetic Valves Ampicillin 2gm IV q4h for 4-6 weeks Penicillin Allergy: *To maximize synergistic effect,
Sensitive to gentamicin PLUS Vancomycin 25-30mg/kg loading administer gentamicin at the same
Gentamicin 1mg/kg IV q8h dose then 15-20mg/kg IV q12h for 6 time close to ampicillin
weeks
Native valve:
Resistant to gentamicin Ampicillin 2g q4h PLUS Symptoms < 3 months – 4 weeks
PLUS Gentamicin 1mg/kg IV q8h for 6 therapy
Ceftriaxone 2g q12h weeks Symptoms > 3 months or prosthetic
valve – 6 weeks therapy
HPP AMG Cardiovascular Infections 21