
Page 180 - HPP ANTIMICROBIAL GUIDELINE 2018
P. 180
Suggested Treatment
Infection/ Condition Comments
Preferred Alternative
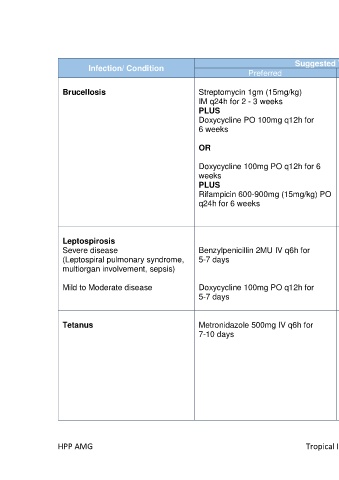
Brucellosis Streptomycin 1gm (15mg/kg) Gentamicin 5mg/kg/24h IV for Longer duration (up to 12 weeks)
IM q24h for 2 - 3 weeks 7 days maybe required in spondylitis,
PLUS PLUS neurobrusellosis, IE, localized
Doxycycline PO 100mg q12h for Doxycycline 100mg PO q12h for suppurated lesions. Please discuss
6 weeks 6 weeks with ID specialists.
OR OR ƚ Recommended alternative for
pregnant woman
Doxycycline 100mg PO q12h for 6 Rifampicin 600-900mg (15mg/kg)
weeks PO q24h for 6 weeks Prophylaxis for laboratory exposure:
ƚ
PLUS PLUS Doxycycline + rifampicin for 3 weeks.
Rifampicin 600-900mg (15mg/kg) PO Trimethoprim/sulfamethoxazole For pregnant, bactrim + rifampicin 3
q24h for 6 weeks (80/400mg) PO 2 tabs q12h for weeks.
6 weeks ƚ
Leptospirosis
Severe disease Benzylpenicillin 2MU IV q6h for Ceftriaxone 1-2gm IV q24h Jarisch-Herxheimer reaction may
(Leptospiral pulmonary syndrome, 5-7 days (If penicillin allergy) occur upon initiation of antimicrobial
multiorgan involvement, sepsis)
Mild to Moderate disease Doxycycline 100mg PO q12h for Azithromycin 500mg PO q24h for
5-7 days 3 days
Tetanus Metronidazole 500mg IV q6h for Benzylpenicillin 2MU IV q6h for Human tetanus immunoglobulin
7-10 days 7-10 days 3000- 6000 units IM stat
At a different site initiate age
appropriate active immunization
All patients with tetanus should
undergo wound debridement to
eradicate spores and necrotic tissue
HPP AMG Tropical Infections 85