
Page 231 - HPP ANTIMICROBIAL GUIDELINE 2018
P. 231
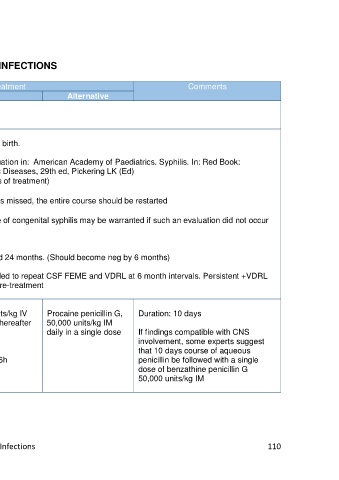
NEONATAL INFECTIONS
Infection/Condition Suggested Treatment Comments
Preferred Alternative
Congenital & Perinatal Infections
Congenital Syphilis Only severe cases are clinically apparent at birth.
T. pallidum
Refer to algorithm for diagnosing and evaluation in: American Academy of Paediatrics. Syphilis. In: Red Book:
2012 Report of the Committee on Infectious Diseases, 29th ed, Pickering LK (Ed)
• Isolate till non-infectious (at least 24 hours of treatment)
• Screen for other STDs and HIV
• If more than one day of penicillin therapy is missed, the entire course should be restarted
• Investigate and treat parents
• Evaluation of the siblings of an index case of congenital syphilis may be warranted if such an evaluation did not occur
previously
Follow-up:
Nontreponemal serologic tests at 3,6,12 and 24 months. (Should become neg by 6 months)
For those with abnormal CSF – recommended to repeat CSF FEME and VDRL at 6 month intervals. Persistent +VDRL
of CSF requires re-evaluation and possible re-treatment
Aqueous crystalline penicillin G: 50,000 units/kg IV Procaine penicillin G, Duration: 10 days
q12h during the first 7 days of life and q8h thereafter 50,000 units/kg IM
daily in a single dose If findings compatible with CNS
involvement, some experts suggest
that 10 days course of aqueous
If diagnosed with congenital Aqueous penicillin G 50,000 units/kg IV q4-6h penicillin be followed with a single
syphilis after one month of age: dose of benzathine penicillin G
50,000 units/kg IM
HPP AMG Neonatal Infections 110