
Page 245 - HPP ANTIMICROBIAL GUIDELINE 2018
P. 245
OCULAR INFECTIONS
Suggested Treatment
Infection/Condition Comments
Preferred Alternative
Preseptal cellulitis
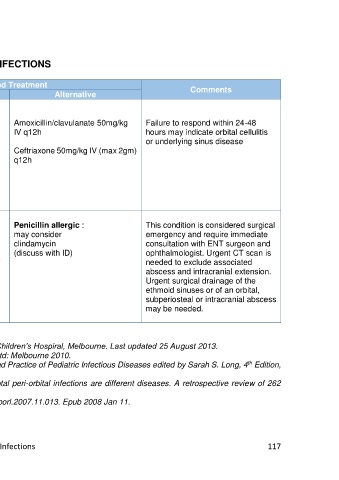
Strep pneumoniae, Staph aureus, Amoxicillin/clavulanate 22.5mg/kg Amoxicillin/clavulanate 50mg/kg Failure to respond within 24-48
Streptococcus ssp. PO q12h for 5-7 days IV q12h hours may indicate orbital cellulitis
or underlying sinus disease
Systemically unwell Cloxacillin 25-50mg/kg (max 2gm) Ceftriaxone 50mg/kg IV (max 2gm)
IV q6h q12h
PLUS
Cefotaxime 50mg/kg (max 2gm) IV
q8h
Orbital Cellulitis/ Abscess Ceftriaxone 50mg/kg(max 2gm) IV Penicillin allergic : This condition is considered surgical
Strep pyogenes, Strep pneumonia, q12h may consider emergency and require immediate
Staph aureus clindamycin consultation with ENT surgeon and
H. influenza (unvaccinated child or PLUS (discuss with ID) ophthalmologist. Urgent CT scan is
untypeable strains) Cloxacillin 50mg/kg (max 2gm) IV needed to exclude associated
q6h for 7-14 days abscess and intracranial extension.
Urgent surgical drainage of the
ethmoid sinuses or of an orbital,
subperiosteal or intracranial abscess
may be needed.
References:
1. Clinical Practice Guideline: Periorbital and orbital cellulitis; The Royal Children’s Hospiral, Melbourne. Last updated 25 August 2013.
2. Therapeutic Guideline: Antibiotics 14 edition. Therapeutic Guideline Ltd: Melbourne 2010.
th
3. Ellen R. W. Chapter 87: Periorbital and Orbital Infection in Principles and Practice of Pediatric Infectious Diseases edited by Sarah S. Long, 4 Edition,
th
2012.
4. Botting AM, McIntosh D, Mahadevan M; Paediatric pre- and post-septal peri-orbital infections are different diseases. A retrospective review of 262
cases.
5. Int J Pediatr Otorhinolaryngol. 2008 Mar;72(3):377-83. doi: 10.1016/j.ijporl.2007.11.013. Epub 2008 Jan 11.
HPP AMG Neonatal Infections 117