
Page 261 - HPP ANTIMICROBIAL GUIDELINE 2018
P. 261
SURGICAL INFECTIONS
Suggested Treatment
Infection/Condition Comments
Preferred Alternative
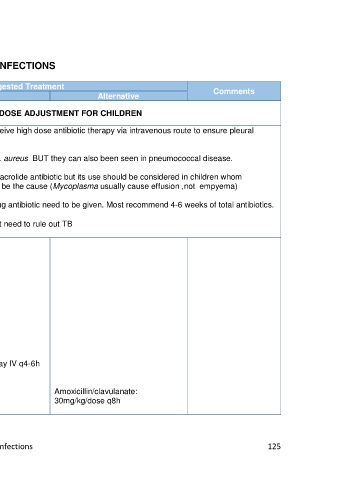
REFER TO ADULT GUIDELINE WITH DOSE ADJUSTMENT FOR CHILDREN
Empyema thoracis All children with empyema need to receive high dose antibiotic therapy via intravenous route to ensure pleural
(Lung empyema): penetration
Staphylococcus aureus
Streptococcus pneumonia Pneumatocele on CXR indicate Staph. aureus BUT they can also been seen in pneumococcal disease.
Empiric treatment: There is NO need to routinely use a macrolide antibiotic but its use should be considered in children whom
Need to cover organisms mentioned Mycoplasma pneumonia is thought to be the cause (Mycoplasma usually cause effusion ,not empyema)
above.
Other bacteria implicated: There is NO CONSENSUS on how long antibiotic need to be given. Most recommend 4-6 weeks of total antibiotics.
Streptococcus pyogenes,
Haemophilus influenza, other gram • In patients not responding to treatment need to rule out TB
negative organisms in
immunocompromised individuals
(empirical)
Cefuroxime 50mg/kg/dose IV q8h
OR
Ceftriaxone 50mg/kg IV q12h
PLUS
Cloxacillin 50mg/kg/dose IV q6h
(if Staph aureus suspected)
Staph aureus (methicillin sensitive): Cloxacillin 50mg/kg/dose IV q6h
Streptococcus pneumonia Benzylpenicillin 200-400,000 MU/kg/day IV q4-6h
(penicillin sensitive):
Streptococcus pneumonia Ceftriaxone 50mg/kg IV q12h Amoxicillin/clavulanate:
(penicillin resistant): (refer to MIC result) 30mg/kg/dose q8h
HPP AMG Surgical Infections 125