
Page 86 - HPP ANTIMICROBIAL GUIDELINE 2018
P. 86
10. Consider adding antifungal therapy if fever persisted or evidence of new infection after 5 to 7 days of broad spectrum antibiotic
therapy or earlier especially in the presence of severe mucositis, oral thrush, painful swallowing, suspicious skin infiltrates or
pulmonary infiltrates, fundal exudates or prolonged steroid/antibiotic use more than 2 weeks.
a. Amphotericin B remains the empirical therapy of choice for invasive fungal infections.
b. For patients who are intolerant, refractory or those with toxicity to conventional Amphotericin B, the lipid formulations of
amphotericin B, voriconazole and echinocandins are alternatives empirical therapy based on local availability and costs.
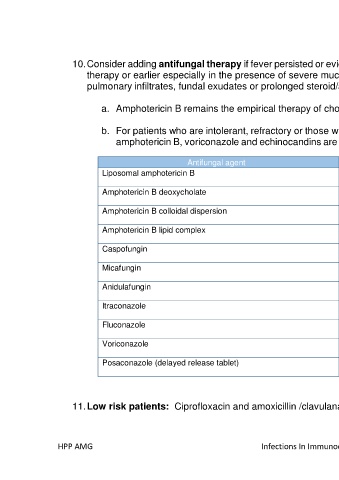
Antifungal agent Dose
Liposomal amphotericin B 3 mg/ kg/ day
Amphotericin B deoxycholate 0.5-1 mg/kg/ day
Amphotericin B colloidal dispersion 4 mg/kg/ day
Amphotericin B lipid complex 5 mg/kg/ day
Caspofungin Load 70mg followed by 50 mg daily
Micafungin Load 200mg followed by 100mg daily
Anidulafungin Load 200mg followed by 100mg daily
Itraconazole 200 mg q12h
Fluconazole Load 800mg followed by 400 mg daily
Voriconazole 6 mg/kg q12h followed by 4 mg/kg q12h
Posaconazole (delayed release tablet) Load 300 mg q12h then 300mg daily ( with food)
11. Low risk patients: Ciprofloxacin and amoxicillin /clavulanate, may be considered after careful assessment.
HPP AMG Infections In Immunocompromised Patients 38