
Page 69 - HPP ANTIMICROBIAL GUIDELINE 2018
P. 69
Suggested Treatment
Infection/ Condition Comments
Preferred Alternative
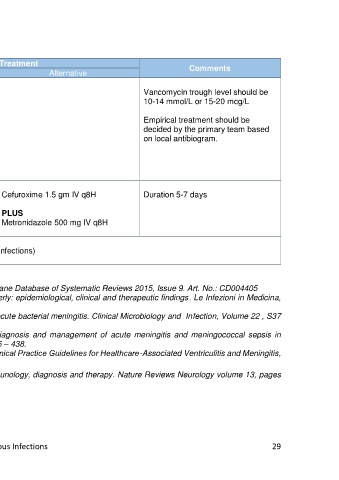
Healthcare-associated Vancomycin 25-30mg/kg loading Vancomycin trough level should be
ventriculitis and meningitis dose then 15mg/kg IV q12h 10-14 mmol/L or 15-20 mcg/L
(not to exceed 2gm per dose)
Empirical treatment should be
PLUS decided by the primary team based
on local antibiogram.
Ceftazidime 2 gm IV q8h
OR
Meropenem 2 gm IV q8h
Cranial trauma Amoxicillin/clavulanic acid 1.2gm IV Cefuroxime 1.5 gm IV q8H Duration 5-7 days
Open fracture q8H
Penetrating injuries PLUS
Metronidazole 500 mg IV q8H
Neurosyphilis Refer to section (Sexually Transmitted Infections)
Reference:
1. Brouwer MC et al. Corticosteroids for acute bacterial meningitis. Cochrane Database of Systematic Reviews 2015, Issue 9. Art. No.: CD004405
2. Pasquale Pagliano et al. Listeria monocytogenes meningitis in the elderly: epidemiological, clinical and therapeutic findings. Le Infezioni in Medicina,
n. 2, 105-111, 2016
3. van de Beek, D. et al. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clinical Microbiology and Infection, Volume 22 , S37
- S62
4. McGill, F. et al. The UK joint specialist societies guideline on the diagnosis and management of acute meningitis and meningococcal sepsis in
immunocompetent adults. Journal of Infection, Volume 7 , Issue 4 , 405 – 438.
5. Allan R. Tunkel et al. 2017 Infectious Diseases Society of America’s Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis,
Clinical Infectious Diseases, Volume 64, Issue 6, 15 March 2017,
6. Peter R. Williamson et al. Cryptococcal meningitis: epidemiology, immunology, diagnosis and therapy. Nature Reviews Neurology volume 13, pages
13–24 (2017)
7. The Sanford Guide to Antimicrobial Therapy 2018
HPP AMG Central Nervous Infections 29