
Page 210 - HPP ANTIMICROBIAL GUIDELINE 2018
P. 210
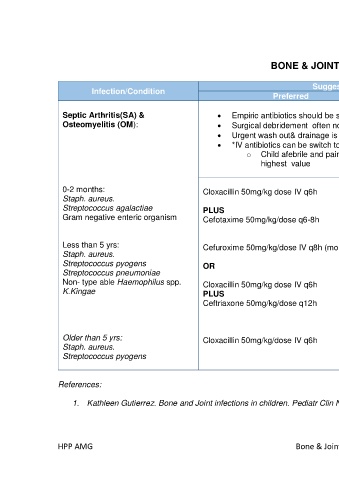
BONE & JOINTS INFECTIONS
Suggested Treatment
Infection/Condition Comments
Preferred Alternative
Septic Arthritis(SA) & • Empiric antibiotics should be started based on clinical diagnosis of SA or OM
Osteomyelitis (OM): • Surgical debridement often not required in OM
• Urgent wash out& drainage is needed in SA in hip and other joints to reduce pressure on growth plate
• *IV antibiotics can be switch to oral if no concurrent bacteraemia when:
o Child afebrile and pain free for at least 24 hrs and CRP <20mg/L or CRP decreased by≥2/3 of
highest value
0-2 months: Cloxacillin 50mg/kg dose IV q6h Amoxicillin/clavulanate 30- Duration of antibiotics:
Staph. aureus. 50mg/kg/dose IV q8h SA: total of 3-4 weeks
Streptococcus agalactiae PLUS (based on amoxicillin dose) OM: 4-6 weeks
Gram negative enteric organism Cefotaxime 50mg/kg/dose q6-8h
Cefazolin 25mg/kg/dose IV q8h In complex disease
Can be use in children with (multifocal, significant bone
Less than 5 yrs: Cefuroxime 50mg/kg/dose IV q8h (monotherapy) suspected Staph aureus or destruction,
Staph. aureus. Strep pyogenes; immunocompromised host
Streptococcus pyogens OR and resistant /unusual
Streptococcus pneumoniae pathogens-need prolonged
Non- type able Haemophilus spp. Cloxacillin 50mg/kg dose IV q6h intravenous antibiotics and
K.Kingae PLUS duration might exceed 6
Ceftriaxone 50mg/kg/dose q12h weeks
Older than 5 yrs: Cloxacillin 50mg/kg/dose IV q6h
Staph. aureus.
Streptococcus pyogens
References:
1. Kathleen Gutierrez. Bone and Joint infections in children. Pediatr Clin N Am 52(2005); 779-794.
HPP AMG Bone & Joints Infections 100